2.23 Dermatofibrosarcoma protuberans
– Raul Valenzuela, MD; Eric Kebbel, Md, MPH
__________________________________________________________________
2.23.1 Background
Dermatofibrosarcoma protuberans (DFSP) is a low-grade malignant tumor arising from dermal and subcutaneous tissues. They make up 6% of soft tissue sarcomas and are the most common cutaneous sarcoma. They are most commonly seen in patients between the ages of 20-50. There is a slight male preponderance.
Up to 50% involve the chest, back, and abdominal wall. The proximal extremities are involved in 35-40% of cases. Head and neck, especially scalp, are also common locations.
DFSP typically presents as a nodular or multinodular cutaneous mass, often with a history of slow but persistent growth. Early lesions may show plaque-like growth with peripheral red discoloration and clinically resemble morphea. May show rapid enlargement due to fibrosarcomatous transformation (in 10-15% of cases).
Treatment is definitive surgical resection, preferably with at least 3cm of clear margins. Local recurrence rates range from 18-55% depending on surgical margins. There is a risk of fibrosarcomatous transformation. Metastases are seen in 3-6% of cases, and are most commonly to lung.
2.23.2 Imaging Features
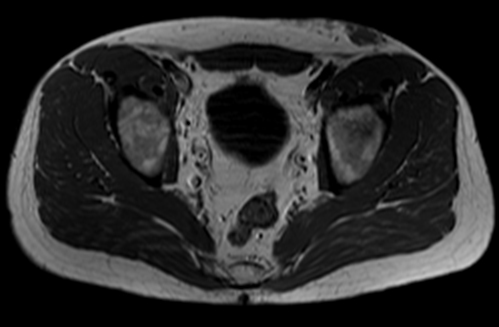
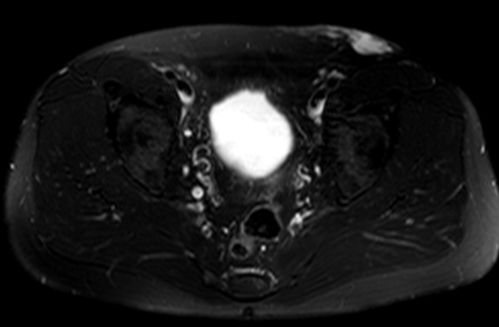
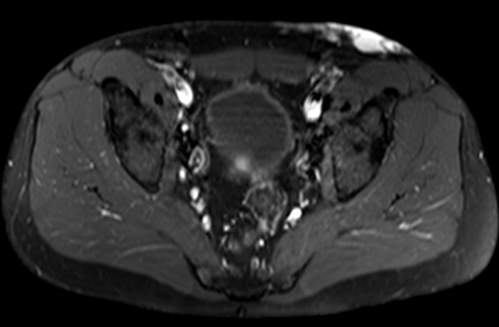
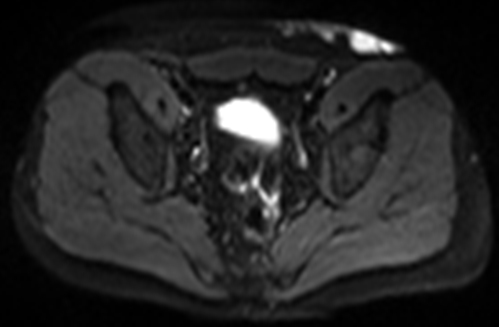
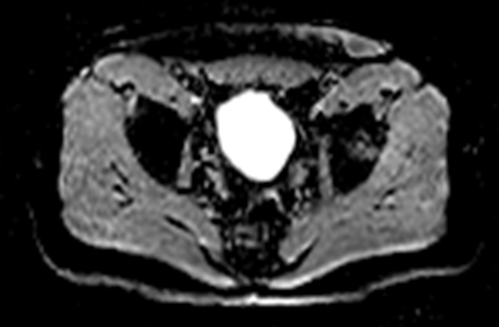
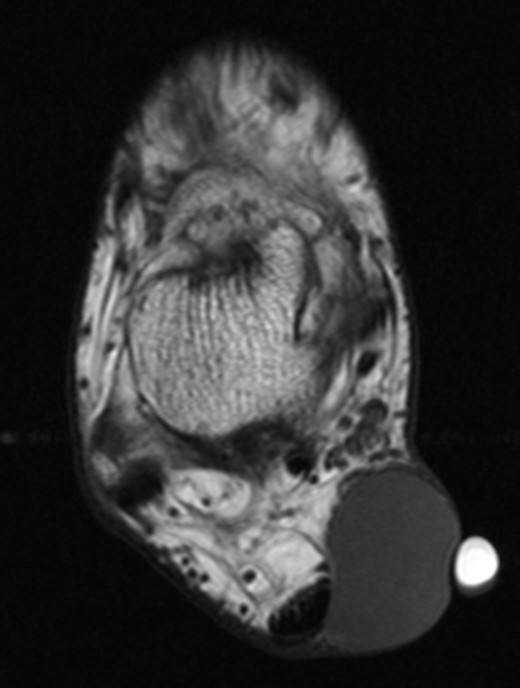
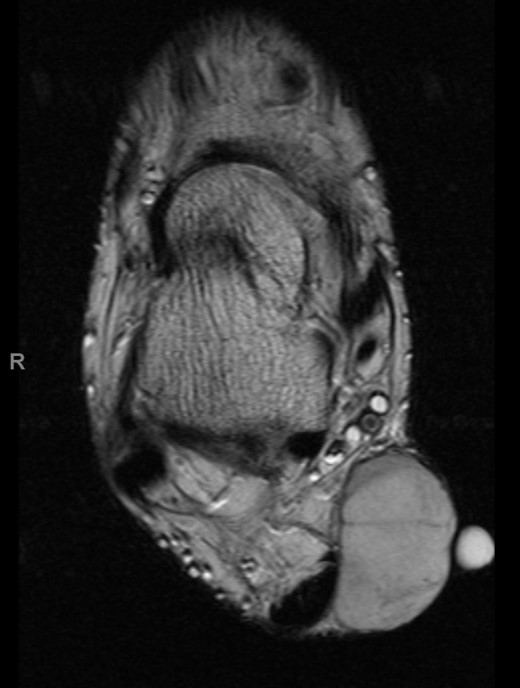
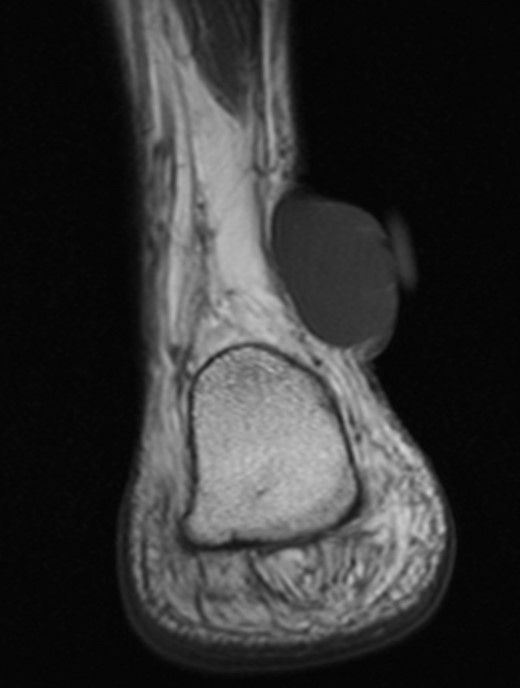
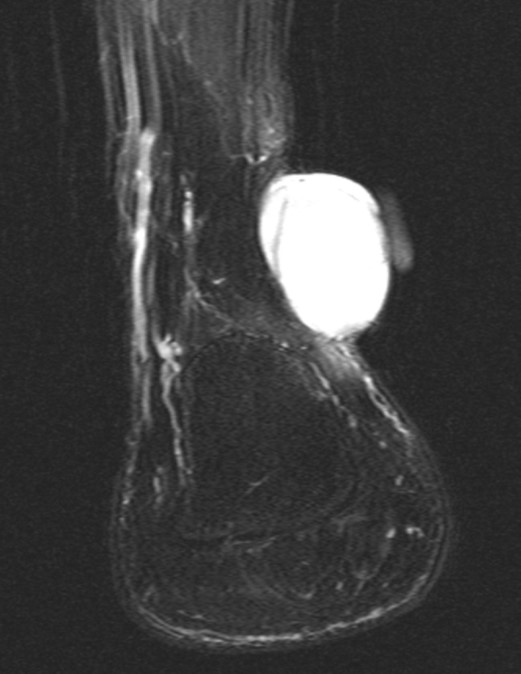
Imaging features can be nonspecific, but should be considered when you see a superficial soft tissue mass. Radiographs and CT may show an exophytic, nodular mass involving skin and subcutis with no calcifications. CT attenuation is similar to muscle. On MRI (Figures 2.1,2.2), the masses are isointense to hyperintense to muscle on T1-WI, hyperintense to muscle on T2-WI, and have moderate to intense contrast enhancement. There may be subcuatenous tails and satellite nodules, with involvement of the skin beyond the nodular mass. The lesions are usually homogeneous, with heterogeneity more commonly seen in larger lesions.
2.23.3 Advanced Knowledge
Several subtypes have been defined. Pigmented DFSP (also known as Bednar tumor) contain a variable number of pigmented, dendritic melanocytic cells. Myxoid DFSP are not common and have prominent myxoid stroma with more nodular growth and numerous vessels with slightly fibrotic vessel walls, often producing a more variable architecture that may mimic other myxoid mesenchymal neoplasms. DFSP with myoid differentiation contain a myointimal, non-neoplastic proliferation in entrapped vessels, with bundles and nests of spindled, myofibroblastic tumor cells. This is more often seen in the fibrosarcomatous variant. Plaque-like DFSP have a flat, plaque-like growth pattern resembling benign plaque-like CD34-positive dermal fibroma. Fibrosarcomatous DFSP represents morphological progression to a usually fascicular pattern with acquisition of metastatic potential. Fibrosarcomatous changes occur de novo or more rarely in local recurrences.
2.23.4 Differential Considerations
Differetial considerations include, neurofibroma, epidermal inclusion cyst, melanoma, basal cell carcinoma, dermatofibroma, desmoid tumor, and epithelioid sarcoma.